In preparing to write this column, I researched the main reasons building owners upgrade the mechanical systems in their commercial buildings. I was dismayed to see that the goal of almost all projects was to decrease operating costs through energy savings. While this is clearly important, as a physician I was hoping to find that more retrofits were being done to improve IAQ for the health of building occupants.
I then remembered an excellent study presented at the Indoor Air 2016 conference in Ghent, Belgium last summer which shed light on this lack of focus on occupant health in commercial buildings. Adams Rackes and his colleagues at Drexel University conducted a survey to see if recommendations on indoor air management to optimize people’s productivity and health were being followed in the U.S. These recommendations were based on years of good research on the relationship between air filtration and ventilation rates and occupant health metrics such as high productivity and low absenteeism from illness. The survey asked over 100 building users, owners, managers, and architectural and mechanical designers about their awareness of and opinions on the health benefits, retrofit costs, and willingness to pay for mechanical systems which would deliver the recommended air treatment.
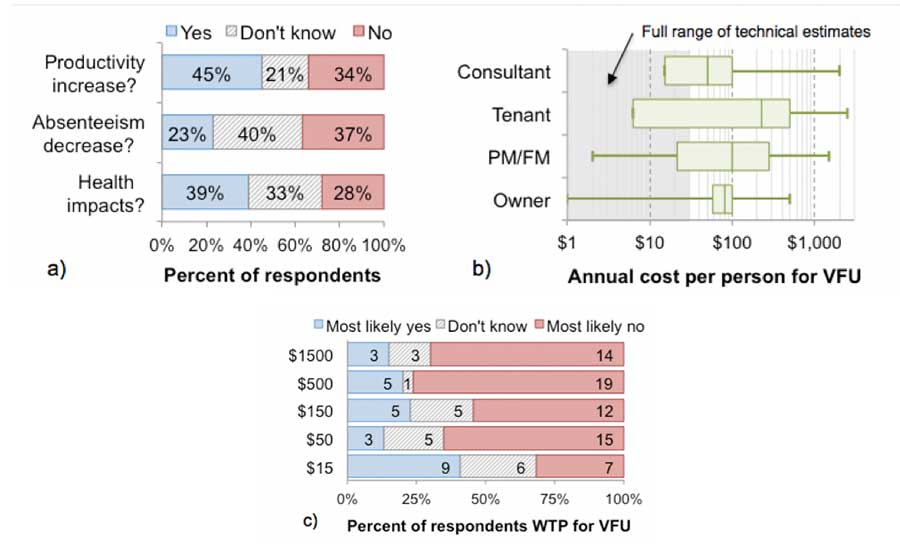
This study revealed a bad situation! Most of the building owners and decisionmakers were either unaware of, or either disagreed with, valid scientific conclusions that optimal ventilation rates and effective filtration would result in the published findings on improved occupant health. While they downplayed the health benefits of good IAQ, they greatly overestimated the costs of the mechanical upgrades and said that no one would be willing to pay the cost to improve IAQ just for occupant health.
Were these stakeholders simply unaware of the scientific associations between IAQ and health? Unfortunately, this did not seem to be the case. Despite having been educated, tested, and certified on their understanding of the scientific data, those holding green building certifications were no more likely to acknowledge any health benefits of increased ventilation or filtration — and were actually less likely to be willing to pay for the mechanical units.
The survey also uncovered significant differences in attitudes between building users and those responsible for costs of the retrofits and operations. People who occupied the building were more likely than owners or consultants to acknowledge IAQ benefits on occupant productivity. In addition, owner estimates of the annual cost per person of the interventions for health greatly exceeded accurate estimates and their willingness to pay for the ventilation systems was low and unrelated to perceived costs.
What is the solution given that the almighty dollar clearly guides decisions about indoor air management? Somehow, clear profitability needs to be built into managing IAQ for human health, not just for building operating costs. The building occupants who are directly affected by IAQ need the education to understand, tools to monitor, and ability to relate IAQ to their health. The next generation of cell phones and wearable fitness trackers need to have the ability to monitor all important indoor components, especially ones that cannot be perceived by human senses, rather than just parameters related to comfort.
For example, low indoor relative humidity and excessive fine particulate matter levels, which are known to be unhealthy, need to be openly and clearly monitored in addition to temperature. Perhaps when building occupants have awareness and a strong voice, either top-down through concerned managers or from a grassroots occupant legal movement, building owners will pay money for healthy humans.



