





The world is just starting to recover from the COVID-19 pandemic. Beyond the human cost of more than 8 million infected people with 437,000-plus deaths, the damage to the world economy will take years to recover. The COVID-19 pandemic is the most severe pandemic since the 1918 Spanish flu, which claimed 50 million lives. However, the world has experienced a number of devastating pandemics between 1918 and now (see Table 1).
Additionally, seasonal influenza has caused approximately 303,000 deaths in the U.S. during the past eight years (see Table 2).Is it time the built environment contributes toward mitigating the spread of coronaviruses and influenza? Yes.
Virus and Pandemic Fundamentals
To have total victory over an enemy, one must fully understand and respect the enemy. So, what is a virus and how many viruses are there? It is estimated there are between 320,000 and 1 million different viruses in the world. Of those, there are 219 known viruses that can infect and cause disease in humans.
A virus is a small infectious agent that contains RNA or DNA genetic material and has a protein outer shell. A virus only replicates within the living cell of the host. Once inside a living cell, the virus directs the living cell to produce more viruses. Viruses can infect humans, animals, plants, and microorganisms.
COVID-19 has RNA genetic material and is part of the coronavirus family, which causes respiratory infections. Other coronaviruses include severe acute respiratory syndrome (SARS) and Middle East respiratory syndrome (MERS). Rhinovirus, adenovirus, enterovirus, human metapneumovirus, parainfluenza, and respiratory syncytial virus are other viruses that cause respiratory infections.
Coronaviruses, which are so named due to their protein shell’s spiky projections or “crowns,” are problematic due to the ease they spread from person-to-person.
How Are Humans Infected by Viruses?
Most viruses do not infect or cause disease in humans. The pathogen pyramid (see Figure 1) illustrates the interaction viruses have with humans.
- Level 1 represents humans being exposed to many viruses. The source of exposure is typically other animals or insects. Most of these exposures do not create infections or disease in humans.
- Level 2 represents the subset of viruses that “jump” from insects or animals to humans causing infections and disease.
- Level 3 represents a subset of viruses that can be transmitted from person to person.
- Level 4 represents a subset of viruses that are easily transmittable (Ro >1. See discussion below) person to person with the potential of causing a pandemic.
The transmission mechanisms for human infection by viruses are as follows:
- Being bitten by infected insect or animal;
- Coming in contact with infected human/animal fluids (blood, saliva, feces, etc.);
- Coming in contact with infected human/animal;
- Coming in contact with contaminated surface;
- Coming in contact/consuming contaminated food/drink;
- Breathing in droplets containing virus; and
- Breathing in aerosol containing virus.
For the general population, the prominent COVID-19 transmission mechanisms are touching an infected person and then touching your nose/mouth, touching a contaminated surface and then your touching nose/mouth, or breathing in droplets containing the virus. It is suspected people are being infected by a transmission that involves a breathing-in-aersol-containing-the-virus mechanism. Beyond the initial virus “jump” to humans, no infected insect or animal to human virus transmission mechanism has been observed. No consumed contaminated food/drink transmission mechanism has been observed.
How do sneezing, coughing, and breathing affect the spread of coronavirus?
It is known that infected people can transmit COVID-19 through particulate generated by unguarded sneezing and coughing. It is suspected that infected people can transmit COVID-19 through breathing. The concern is contaminated particles stay aloft long enough to be subsequently breathed in by another person, infecting them. The size of a particle determines how long the particle will stay aloft (see Table 4). A large 100-micrometer (µm) particle will stay aloft 4.9 seconds while a 1-µm particle will stay aloft 12 hours. Table 4 particle aloft times are based upon still air. Indoor supply air diffuser induction airflow extends particle aloft time. The World Health Organization considers particles larger than 5 µm a droplet and particles smaller than 5 µm aerosol. The number and size of particles generated by coughing, sneezing, and breathing are as follows:
- Coughing generates approximately 75,400 particles/cough in the 0.35 µm to 10 µm size range with the majority of the particles generated in the 0.35-1.5 µm size range. Cough-generated aerosol will stay aloft for up to two days.
- Sneezing generates approximately 40,000 particles/sneeze in the 7-2,000 µm size range with the average particle size of 74 µm. Sneeze generated droplets will stay aloft up to 33 minutes.
- Breathing generates approximately 250 particles per breath in the 0.3-20 µm size range with the majority of the particles generated below 1 µm. Breath-generated particles will stay aloft for two days.
How Contagious are Viruses?
The medical community has developed a mathematical term (Ro) that shows how contagious a pathogen is. Ro (R naught), is the basic reproduction number that indicates how contagious or transmissible an infectious disease or parasitic agent is. Ro indicates the average number of people a contagious individual will infect.
- Ro below 1 indicates a contagious individual will transmit the disease to less than one person. The disease will decline and die out.
- Ro equal to 1 indicates a contagious individual will transmit the disease to just one person. The disease will spread but not create a pandemic.
- Ro above 1 indicates a contagious individual will transmit the disease to multiple people. The disease spreads easily from person to person with the potential of a pandemic.
Ro is based upon the disease being new with no available vaccination or method to control its spread. There are other variables that affect Ro values that can be found in a Centers for Disease Control and Prevention (CDC) perspective article, “Complexity of the Basic Reproduction Number.”
Table 3 provides a list of infections with their corresponding Ro ranges. The COVID-19 Ro range is 1.47-2.59, which is similar to the 1918 influenza outbreak and seasonal influenza.
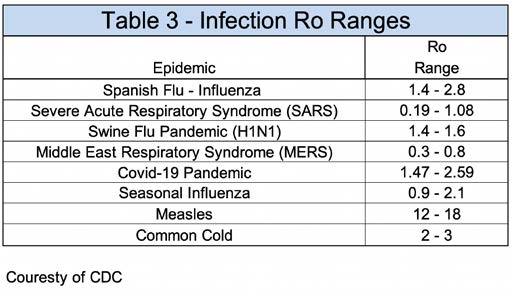
Influenza Ro Ranges.
What Are the Stages of a Coronavirus Pandemic?
The CDC developed a framework that describes the six stages of a coronavirus pandemic (see Figure 2) and their response during each stage. The six stages are as follows:
-
Stage 1 – Investigation Stage: Identification and investigation of a novel coronavirus infection that is believed to have potential implications for human health. Can be a single or handful of individuals or animals.
-
Stage 2 – Recognition Stage: Initiated when increasing numbers of human cases with novel coronavirus infection with the virus characteristics indicating an increased potential for ongoing person-to-person transmission.
-
Stage 3 – Initiation Stage: Indicated by human cases anywhere in the world with demonstrated efficient and sustained person-to-person transmission.
-
Stage 4 – Acceleration Stage: Indicated by consistently increasing rate of coronavirus infection cases.
-
Stage 5 – Deceleration Stage: Indicated by a consistently decreasing rate of coronavirus infection cases.
-
Stage 6 – Preparation Stage: Indicated by low coronavirus infection activity. Resuming enhanced surveillance protocols to detect subsequent waves of infection.
Environmental Impact on Coronavirus
How does temperature and relative humidity affect coronavirus? The influence air temperature and relative humidity has on COVID-19 transmission is in the early stages of research. One preliminary study, “High Temperature and High Relative Humidity Reduce the Transmission of COVID-19,” indicated the COVID-19 Ro value dropped by 0.0212 for every degree Fahrenheit (0.0383 for degree Celsius) increase in temperature and dropped by 0.0224 for every percentage relative humidity increase. This study was based upon outdoor temperatures and relative humidities. The study did not address corresponding indoor temperatures/relative humidities and how temperature/relative humidity affects human immune systems. Addressing these variables will require a long-term study.
At lower space relative humidities, generated particles will partially desiccate and become smaller particles, which extends the time frame they remain aloft. The partially evaporated particle has a greater opportunity to infect a person.
Relative humidity affects the respiratory system’s defense mechanism. One respiratory system defense mechanism protects the lungs from pathogens and consists of cilia and a mucus layer. The mucus layer traps pathogens, preventing them from reaching the lungs. The cilia are small, hair-like projections that move the mucus layer upward in the trachea to be coughed out or swallowed. The respiratory system has other defense mechanisms (e.g. inferon). At higher relative humidities, the respiratory defense system is efficient at removing pathogens and preventing infections. At lower relative humidities, the respiratory defense mechanism is less efficient, making the lungs more susceptible to infection.
The optimum relative humidity range is 40%-60% to prevent the desiccation of projected particles and to have an optimum respiratory system defense system.
COVID-19 was found to be viable for four hours on copper, 24 hours on cardboard, 72 hours on plastic, and 72 hours on stainless steel. At the time of writing this article, no testing data was available for glass, wood, stone (marble, granite), nickel, or painted surfaces.
Mitigation Options
Though person-to-person interaction and personal hygiene are the most influential in reducing a virus outbreak, the built environment can provide substantial support in infection control.
The built environment’s most limiting factor in supporting coronavirus outbreak mitigation is that 80%-90% of the buildings that will exist in our lifetime are already built. Most existing building owners want to incorporate building system modifications that provide the best mitigation for the least amount of capital investment and disruption to tenants. Incorporating modifications to residential structures may be problematic due to an owner’s inability to pay for modifications.
Providing multilayer infection control modifications to the built environment will support mitigating the coronavirus. Some potential modifications include no-touch operation, added humidification to the HVAC system, the installation of higher efficiency filters, increased space airflow, improved airflow directionality, dedicated work station supply air, the addition of upper room and/or air-handling-unit ultra-violet lighting, and increased outdoor airflow.
The indoor areas, where someone has the highest potential of contracting an infection, are high-density occupancy areas (conference rooms, auditoriums, restaurants, breakrooms, arenas) and transient spaces (elevators, stairs, corridors/hallways, aisles) and should be the primary focus for coronavirus mitigation modifications.
No-Touch Operations — No-touch faucets are common in commercial restrooms, and automatic doors are common at grocery store entrances. Automatic door operation can be extended to other doors, especially restroom doors. A voice-activated control system could be used to activate various building system operations (e.g., tell elevator which floor you want to go to, tell thermostat to raise/lower space temperature). For surfaces that are frequently touched, consider using copper or copper coated material.
Add Humidification to the HVAC System — Preliminary studies show that humans have better immune systems when in higher relative humidity environments (40%-60%), resulting in a reduced spread of a coronavirus. It has not been determined whether the better immunity response is based upon just having humidification in the work environment or if both the residence and work environments need humidification.
The most convenient location to install humidification is the air-handling unit. Unfortunately, most air-handling units that were not designed with humidification probably do not have adequate space to install humidification. The humidification may have to be duct-mounted or installed within the occupied space.
If humidification is being added to a building, it is important to evaluate the impact humidification has on the building envelope vapor diffusion and liquid transport. Adding humidification may severely damage materials within the building envelope. There are computer software packages (i.e. WUFI) available that can calculate the impact of adding humidification to a building.
Install Higher Efficiency Filters — Most building HVAC systems have MERV-7 or MERV-8 filters installed. These filters have 25%-35% dust spot efficiency, which is good for large particle contamination but not efficient at removing smaller particles containing a pathogen. Adding higher efficiency filters (MERV 13 or MERV 14) to the HVAC system can remove particles infected with a coronavirus. MERV 13 and MERV 14 filters have 90%-95% dust spot efficiency.
The original MERV 7 or MERV 8 filters will need to remain as prefilters and the MERV 13 or MERV 14 filters should be added downstream of the prefilter. The HVAC system will need to be evaluated for adequate space to install the higher efficiency filters and the impact the additional filter static-pressure drop has on the HVAC system airflow capacity.
Increase Space Airflow — The old saying, “the solution to pollution is dilution” has value in dispersing particles. Hospital operating rooms are very sensitive to viable particles and have a minimum 20 air changes per hour (AC/hr) requirement. A typical office building has approximately 1 cfm per square foot supply air, which translates to 7.5 AC/hr for a space with an 8-foot ceiling. Air change rates in the 12-18 AC/hr range were found to efficiently reduce particle concentrations.
Most existing HVAC systems do not have appreciable excess airflow capacity. Increasing airflow in the high-density occupancy areas and transient spaces should be evaluated. Do HVAC systems have excess airflow capacity? If not, could a recirculation fan with a MERV-13 filter be installed to provide additional ventilation to these spaces?
Elevator cabs have high-density occupancy and poor ventilation. A fan filter unit with MERV-13 filters would take elevator shaft air and supply air at the ceiling. Low wall relief air grilles should be provided to ensure airflow direction goes from ceiling to floor.
Improve Airflow Directionality — In high occupancy and transient spaces, having ceiling supply air with low wall return will reduce particle recirculation. This is a very common design philosophy for operating rooms and cleanrooms.
Dedicated Work Station Supply Air — Most supply air diffusers have high-velocity discharge, which creates an induction air current inside the space (see Figure 3). The induction air current distributes the air within the space and blends the supply air with air within the space to prevent cold air dumping on occupants and hot air remaining stagnant at the ceiling. A supply air diffuser will typically supply an area of 100-300 square foot (9-27 square meters), which can cover a number of cubicles/work stations. All of the air within a diffuser’s area will be recirculated including any pathogens.
An alternative supply air method is to provide a dedicated supply air nozzle at each work station (see Figure 4). The supply air nozzle has a smaller induction area and pulls the induction air from the ceiling instead of the breathing zone. Any pathogens in the supply air will affect a substantially smaller area. The dedicated supply air nozzles will provide occupants the opportunity to adjust their individual work station airflow.
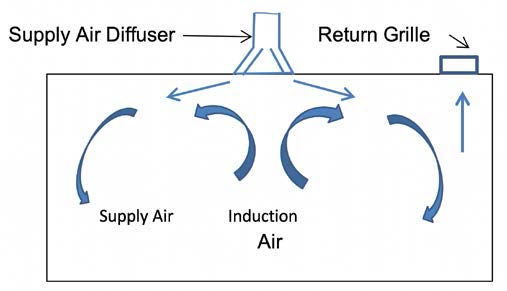
A space airflow pattern with a diffuser.
Install Upper Room and/or Air-Handling Unit Ultraviolet Lighting — Ultraviolet light (UVC) uses short-wave energy to inactivate viruses, bacteria, and fungi so they do not cause disease. Ultraviolet light can be used in the air-handling units to prevent transmission of coronavirus through the HVAC system.
Most supply air diffusers have high-velocity discharge that creates an induction-air current inside the space (see Figure 3). An upper room UVC fixture can inactivate coronaviruses in the supply airstream. The most effective areas to install upper room UVC fixtures are in the high-density occupancy and transient spaces (see Figure 5).
A similar technology to UVC is ionizers, which add an electromagnetic charge to the particles that flow through it. These charged particles are attracted to other particles, which become heavier and have a shorter aloft time. The disadvantage for ionizers is that they contain a virus instead of inactivate them. Another concern with ionizers is the level of generated ozone. Ozone can damage occupant lungs.
Increase Outdoor Airflow — Modifying an HVAC system from partial outdoor airflow to 100% outside airflow will more efficiently flush a pathogen out of the building. It is important to verify that a system enthalpy wheel is bypassed on the exhaust side to prevent the re-introduction of pathogens into the HVAC system. The HVAC system heating coil and cooling coil capacities need to be verified that they can maintain space conditions with the higher outdoor airflow. There will be a large increase in the building’s energy usage but it is effective at removing pathogens during a pandemic.
Research has shown that elevated air CO2 concentrations (>5,000 ppm) cause high blood CO2 levels (hypercapnia), which research has shown causes suppressed immune function. No research was found showing if immune system suppression occurs at lower CO2 concentrations. It is recommended immune function research be performed at CO2 concentrations normally experienced during demand ventilation (~1,500 ppm).
Conclusions
The coronavirus is a wake-up call that the built environment lacks adequate infection control measures to mitigate the spread of pathogens.
Implementing a multilayered mitigation plan can substantially support the reduction of coronavirus transmission. No-touch doors, humidification, ultraviolet lighting, and higher efficiency filters will provide the best results with the least disruption to the building occupants.
It is recommended that research be performed to determine the effectiveness of each mitigation measure. The mitigation measures that prove effective should be considered for inclusion in the building codes.




