
The National Fire Protection Association (NFPA) 99 is a code that sets vital health care safety regulations for the protection of patients, staff, and the general public within health care facilities. It addresses various areas, including requirements for the design of HVAC systems. Specifically, paragraph 9.3.1.1 of NFPA 99 mandates compliance with ASHRAE Standard 170 – Ventilation of Healthcare facilities, formally referred to as ANSI/ASHRAE/ASHE Standard 170.
The Facility Guidelines Institute (FGI) is responsible for formulating comprehensive guidelines for the planning, design, and construction of hospitals, outpatient facilities, and residential health care and support facilities. To ensure a unified approach to health care facility planning, design, and construction, FGI guidelines incorporate and align with key safety and environmental health standards, including those defined by the NFPA 99 code and ANSI/ASHRAE/ASHE 170 standard.
FGI's integration of the ANSI/ASHRAE/ASHE Standard 170 - Ventilation of Health Care Facilities in its 2010 edition of the guidelines highlights the importance of this standard in shaping health care facility design. As stated in an excerpt from FGI, "Beginning with the 2010 Guidelines edition, ANSI/ASHRAE/ASHE Standard 170 - Ventilation of Health Care Facilities has been incorporated into the Guidelines as minimum requirements for ventilation systems ... ASHRAE keeps Standard 170 under a continuous maintenance process, which permits official changes to be made at any point over the life cycle of the document."
This strong emphasis on ANSI/ASHRAE/ASHE 170 reveals its integral role in shaping the ventilation standards upheld by FGI. As part of their continuous maintenance process, ASHRAE provides regular updates to Standard 170, ensuring that the guidelines remain in sync with the latest knowledge and best practices in the design and operation of ventilation systems in health care facilities.
ANSI/ASHRAE/ASHE 170 is an integral reference in the realm of HVAC systems within health care settings, providing detailed specifications for ventilation and air filtration. It delineates unique filtration requirements based on distinct space types in health care facilities, such as operating rooms, patient rooms, laboratories, and more. These guidelines are meticulously laid out to address airborne contaminants and infections, ensuring each space has appropriate air quality measures in place. The convergence of NFPA 99, FGI, and ASHRAE 170 plays a pivotal role in ensuring health care facilities achieve optimum air cleanliness and safety, which directly contributes to overall patient care and wellness. This sets the foundation for our ensuing discussion, where we will delve into the diverse filtration requirements defined by these codes and standards. Additionally, we'll explore various approaches to HVAC system design in the healthcare setting, tailored to meet these stringent requirements while prioritizing patient health and safety.
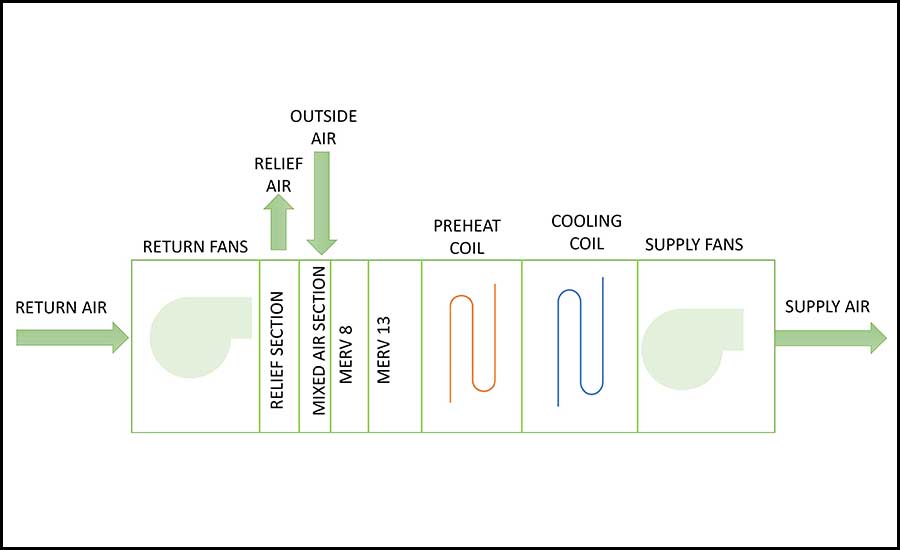
Even though ASHRAE Standard 62.1 - Ventilation for Acceptable Indoor Air Quality requires that HVAC systems that serve commercial-type spaces be provided with a minimum level of filtration of MERV 8, a typical air-handling unit (AHU) serving office-type spaces typically utilizes a two-stage filtration process. As shown in Figure 1, the first stage employs a MERV 8 filter, which effectively removes 70%-85% of larger particles (3-10 microns) from the air. The second stage utilizes a more refined MERV 13 filter, which typically can capture more than 75% of the particles that have a size between 0.3 microns and 1.0 micron.
Paragraph 6.4 - Filtration of ANSI/ASHRAE/ASHE 170 defines specific filtration requirements that HVAC systems serving health care spaces must comply with. Similar to ASHRAE 62.1, note a requires that minimum MERV-8 filters are to “be provided upstream of the first heat exchanger surface of any air conditioning system that combines return air from multiple rooms or introduces outdoor air.” Further, and as stated in an excerpt from the same paragraph, note h requires that “for spaces that do not permit air recirculated by means of room units and have a minimum filter efficiency of MERV-14, MERV-16, or HEPA in accordance with Table 7-1, 8-1, or 8-2, the minimum filter requirement listed in Table 7-1, 8-1, or 8-2 shall be installed downstream of all wet air cooling coils and the supply fan.” Figure 2 shows a sample configuration of an AHU that complies with the requirements stated in note h.
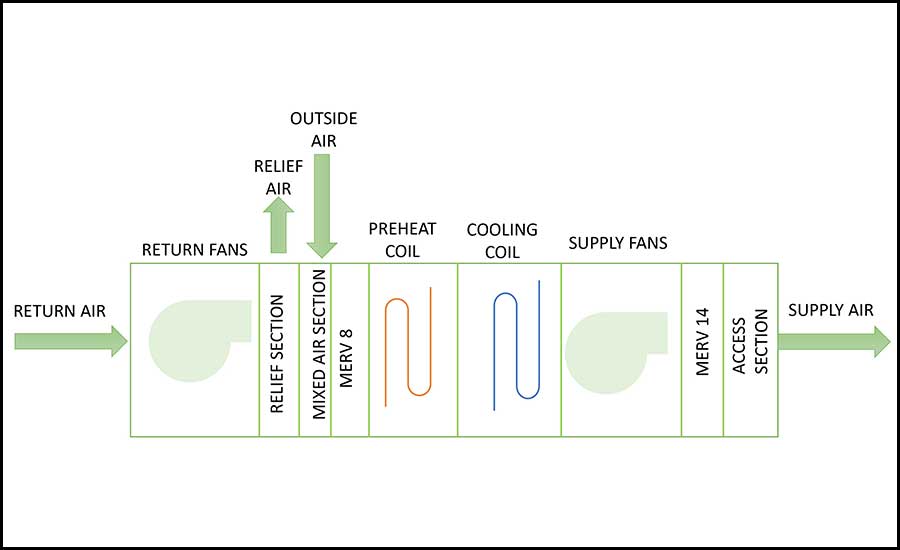
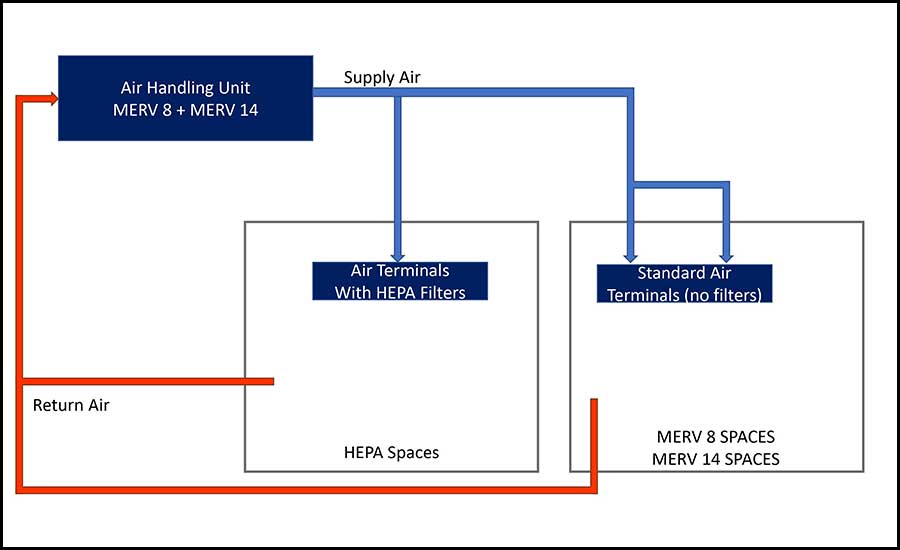
Figure 3 shows a scenario in which an AHU serves multiple types of spaces, as defined by tables 7-1, 8-1, or 8-2, and said spaces have different filtration requirements. A potential design approach that is compliant with ANSI/ASHRAE/ASHE 170 is to design the AHU with MERV 8 as a prefilter and MERV 14 as a final filter; HEPA filters will then be provided as a part of the air terminals that serve the spaces that have more stringent filtration requirements, typically combination AII/PE anterooms, combination AII/PE room, PE anteroom, burn unit, specialized operating rooms and specialized Class 3 imaging rooms.
Even though Table 7-1- Design Parameters— Inpatient Spaces defines the minimum filtration level for operating rooms (ORs) to be MERV 16, this requirement does not apply to all operating rooms; this is because sub-note hh of Table 7-1 refers the designer to Section 7.4.1.c of ANSI/ASHRAE/ASHE 170, which reads “In ORs or Class 3 imaging rooms designated for orthopedic procedures, transplants, neuro surgery, or dedicated burn unit procedures, HEPA filters shall be provided and located in the air terminal device”.
When there is a need for the AHU to provide humidification, the process of determining a location for the humidifier inside of the AHU becomes extremely important; filters, in particular high efficiency filters, can get clogged up by water droplets relatively fast. To prevent this issue from occurring, note c under paragraph 6.4 – Filtration, requires “The design shall include all necessary provisions to prevent moisture accumulating on filters located downstream of cooling coils and humidifiers.” Figure 4 shows a proposed layout of an AHU that is provided with humidification. In this scenario, the humidifier is located downstream of the MERV 8 filter and preheat coil and upstream of the cooling coil, supply fans and final filter. Having the cooling coil downstream of the humidifier ensures that any moisture carryover (from the humidifier) is captured by the coil (and associated drain pan). From the perspective of humification, having the supply fans located downstream of the humidifier will serve at least two purposes: 1) complete mixing of the air and the steam that is being discharged by the humidifier and 2) slightly changing the relative humidity of the airstream by adding sensible heat so that the airstream is no longer close to full saturation.
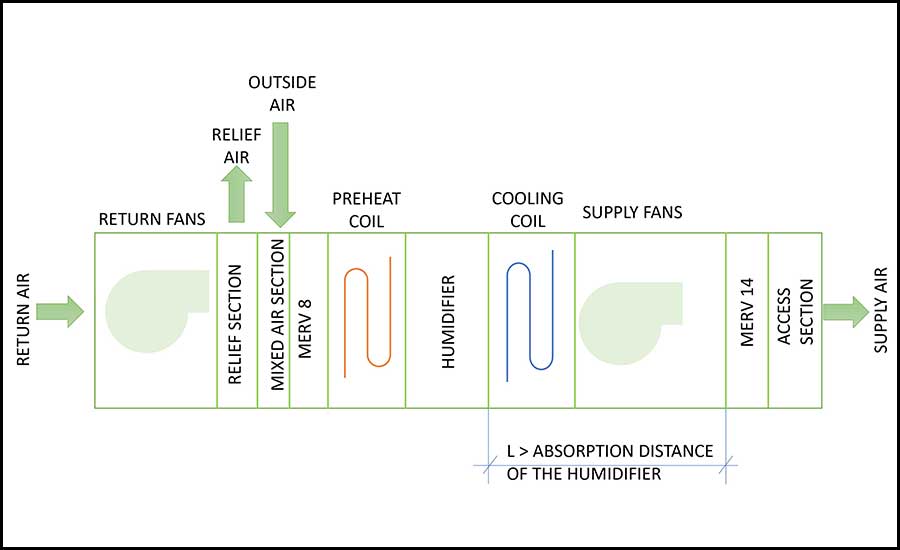
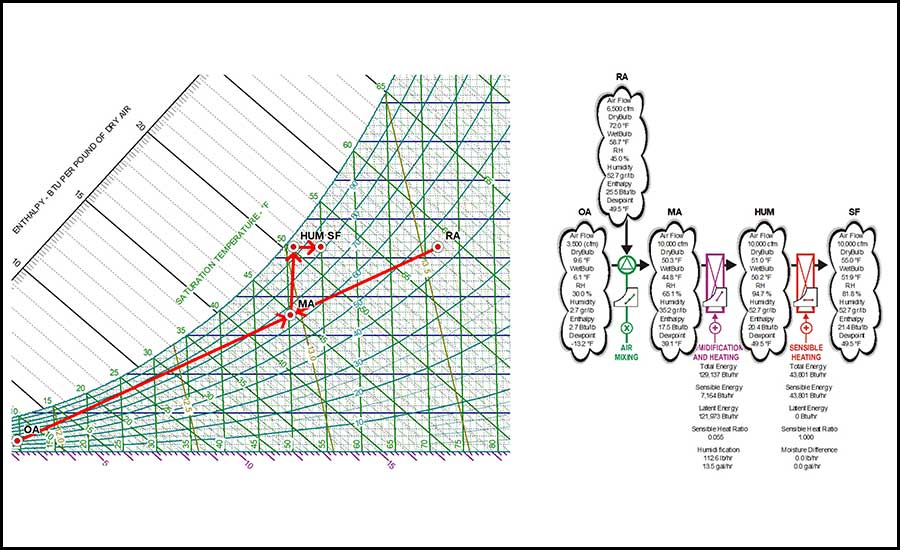
Figure 5 shows a sample psychrometric analysis of an AHU that is provided with humidification and has the final filters located downstream of the supply fan. As shown in the associated flow chart, the sensible heat gain from the supply fans changed the relative humidity of the airstream from 94.7% to 81.8%.
As shown in Figure 6, in some cases, i.e., when the indoor relative humidity (RH) design conditions are high, humidifying the mixed airstream without any preconditioning is not possible. To address this challenge, we will need to change the enthalpy of the mixed air by activating the preheat coil and then the humidifier. Figure 7 shows the associated psychrometric flow chart. By activating the preheat coil and using the sensible heat from the supply fans, the relative humidity of the airstream decreased from saturation levels down to 84.5%, which is a level of relative humidity that does not negatively impact the useful life of the final filters.
As we draw to a close, this author hopes that it has become evident that the selection and positioning of filters in HVAC systems extend beyond mere compliance with codes, such as the ANSI/ASHRAE/ASHE 170 standard. It necessitates a profound understanding of psychrometrics, fan laws, and good design practices to optimize the system's operation. The choice of filter location can significantly impact the efficiency of air filtration, the energy consumption of the system, and the overall health and safety of the indoor environment.
In particular, understanding psychrometrics can guide decisions around humidity control and the necessary preconditioning of air. By managing heat gains and relative humidity in the airstream, we can prevent undue moisture accumulation on filters downstream of cooling coils and humidifiers, enhancing the life and performance of these filters.
Moreover, fan laws dictate how changes in the system, such as added filter resistance, can affect fan performance and power consumption. Being cognizant of these laws helps in making strategic choices that enhance system efficiency while meeting the stipulated air quality standards.
In essence, the design and construction of HVAC systems in health care settings are an intricate science and art, balancing code compliance with the demands of unique space requirements, psychrometrics, and energy conservation principles. Through this comprehensive approach, we can ensure the creation of health care environments that support optimal patient care and wellness.




